
|
PHACOEMULSIFICATION TRAINING PROGRAMME
- Navneet Hospital , Solapur is conducting a training course of one week for doctors from India and two weeks for Doctors from overseas in Phacoemsulsification.
- The training is geared to help the Ophthalmologist who are interested to learn Phaco.
- The course will include – Wet Lab, Lecturers, CD presentation of basic and complicated Phaco surgeries .
- Hands on training
- At a time ONE/TWO candidate
- Course duration – One week for doctors from India and Two weeks for Doctors from overseas
- Facilities available
- Well equipped Operation Theatre
- Two Zeiss operating microscope with CCTV
- Four Phaco Machines
- Soverign Compact White Star from Allergan – USA
- Opsys from Allergan – USA
- Diplomax from Allergan – USA
- Galaxy from Appasamy Associaties – India
- Audiovisual Facility – VCR, DVD/CD player, Laptop, LCD projector.
- Internet Access
- Course Material
- Manual of Basic Phaco
- CD of Basic Phaco
- CD of Complicated cases of Phaco
- CD of your own phaco cases
- Completion Certificate
- Surgical Work
- Wet Lab
- You will get opportunity to do enough number of surgeries until you get confidence.
- Assistant Phaco Training Program --- We have also started 'Assistant Phaco Training Program' for Machine Technician, Ophthalmic Assistant, O.T. Asistant, Nurses, Etc.
Dr. Navneet Toshniwal
Course Director
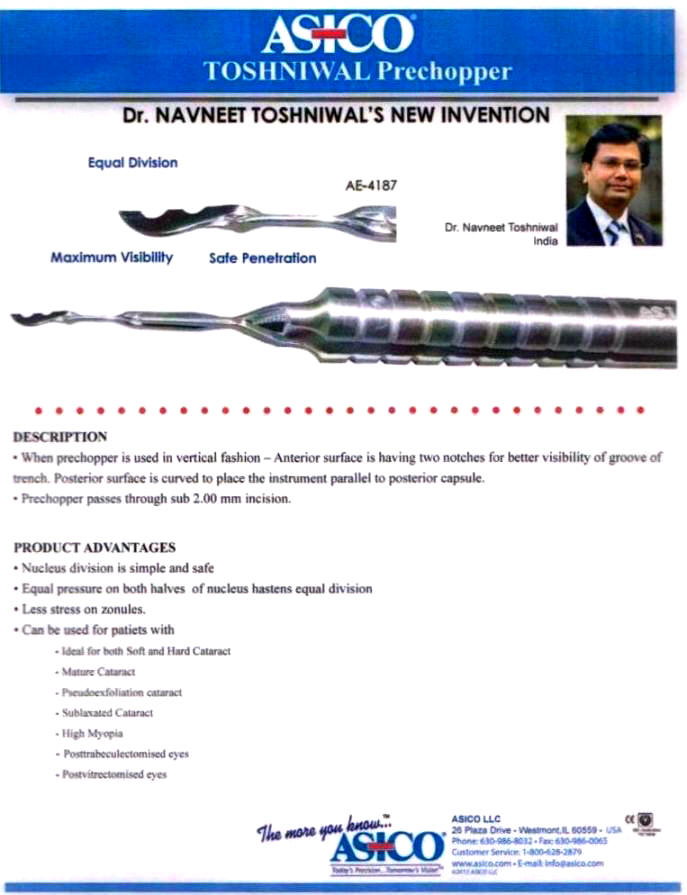
PRECHOPPER
SIMPLIFIED PHACOEMULSIFICATION - Book By Navneet Toshniwal
Please Zoom In to start and better view of Book Brief
.
Introduction
Introduction of Capsular Tension Ring [CTR] is mainly for management of zonular dialysis. In 1991 , Hara et al published "equator ring" for maintenance of the circular contour of capsular bag after IOL removal. They used flexible Silicon rods designed on its undersurface with a groove.
A PCIOL is inserted in the bag with IOL loops in the groove. Equator ring made of PMMA to prevent IOL decent ration. This ring initially designed to inhibit the proliferation of equatorial epithelial cells.
Ledger et al in 1993 presented a film named 'The Capsular Tension Ring' . A new device, for complicated cataract surgery at the third ASCRS at Washington in may 1993. After this many surgeons like Gonni, Gimbel, Osher, Fine used this CTR for patients with zonular weakness.
Indication and Advantages
- CTR is indicated in patients with zonular dehiscence.
- To Maintain circular contour of bag.
- Prevents IOL decentration.
- Prevents posterior capsule opacification by exerting mechanical pressure on equatorial cells and preventing their proliferation and migration.
Different Rings - Size, Shape
Sizes - Diameter of 12 mm compressible to
10 mm i.e. 12/10, 13/11, 14.5/12 Shapes -






Diaphragm -
- Standard CTR - For Moderate zonular dehiscence
- MCTR - Model 1-L - Single fixation hook distant from the insertion end of ring.
- MCTR - Model 2-C - Single fixation hook near the insertion end of the ring.
- MCTR - Model 2-L - Two fixation hooks attached to the CTR . All these MCTR [Modified]. Capsular Tension Ring] is used for severe capsular dehiscence, marfan's syndrome
- CTR with Iris diaphragm - Consist of seven black opaque segments. Uused in Aniridia patients.
- CTR with Coloboma diaphragm. - Designed by Witschel hasa, diameter of 13/11 mm - Black Opque segment of 2.5 mm.Used in Large inidectomy, Iris Coloboma
Technique
- Macpherson forcep
Through main incision or side port or another stab incision near iris diaphragm.
- Injector or shooter.
Capsulorhexis is must for CTR introduction Should be small, continuous and well defined. Start capsulorrhexix away from zonular dehiscence area. In some undiagnosed cases on Slitlamp examination, feeling of capsulorhexix is very important i.e. while doing CCC there is a wrinkling of capsule which indirectly emphasis that there is no stretch over capsule [zonular weakness] . In such situation you can put CTR on prevention basis.
- CTR is introduced in different situation in
Phaco procedures.
- Before Nucleus delivery which is already
decided
Procedure - Make a good pocket between capsule and nucleus by viscoelastic and then put CTR by Forcep or injector.
- During Nucleus management
While doing procedure CTR may required after trenching of nucleus ,after division of nucleus, during chop procedure. Because of lack knowledge of parameters of Phaco , improper handling of instrument can cause zonular dehiscence in all mentioned conditions.
- During Irrigation and aspiration of epinucleus
and cortex
Removal of cortex which is stucked in CTR is and art - Aspiration of Cortex must be done in a tangential manner from equator.
- After insertion of IOL - For better centration
of IOL.
Sometime one or two rings may be needed to stabilse the bag.
- In large dehiscence or in marfan's syndrome
MCTR is used.
Before inserting MCTR in the capsular bag, 10-0 prolene suture is preplaced and passed through the eyelet of fixation hook. The fixation hook must be positioned at the side of the zonular dehiscence. The needle of preplaced prolene suture is introduced through the incision, then behind the iris and then penetrates through the scleral wall at the site of fixation hook. The needle should exit the scleral wall opproximately 1.5 mm posterior to corneo-scleral junction. The sutures are tied and adjusted until centration of the capsular bag is achieved. The knot is burried beneath a scleral flap.
- Before Nucleus delivery which is already
decided
Contraindication
CTR is contraindicated - if capsulorrhexix is not complete.- posterior capsule rupture
Complications
- During insertion can cause damage to endothelium
- can increase preexisting capsular dehiscence.
Conclusion
- CTR is one of the important device for phacoprocedure.
- Injector Technique of introducing CTR has changed the scenario of complicated phacoprocedure.